Massively promising news for the cannabis industry today that many are calling historic: the Department of Health and Human Services (HHS) has sent a letter to the Drug Enforcement Administration (DEA), recommending that cannabis be rescheduled from Schedule I to Schedule III. The news was originally reported by Bloomberg, but further expanded on (and without a paywall we’ll add) by Marijuana Moment with comments from the DEA, HHS and the White House.
Many cannabis stocks across the market saw significant spikes in trading prices following the news of the recommendation. Industry stakeholders and trade organizations seem to share a similar sentiment across the board: Not quite exuberance and celebration, but cautious optimism. The move doesn’t mean the federal government is legalizing cannabis, but they are showing their willingness to work with the industry.
The current Schedule I status of cannabis means the DEA and the federal government see no medical value in it and a high potential for abuse, grouping it with heroin and cocaine. Moving it to Schedule III would mean the opposite, that they recognize cannabis does have medical value and does not have a high potential for abuse, which would put cannabis in the same classification as ketamine, testosterone and Tylenol with codeine.
Importantly, the move would remove the dreaded 280E tax burden that has plagued the cannabis industry with huge tax penalties. It would also lift many barriers to study cannabis that have hindered research for decades.
Last year, President Biden asked HHS to review the scheduling of cannabis, and this recommendation letter to the DEA appears to be the culmination of their review. It is only a recommendation and nothing happens instantly. The DEA still has to decide if they choose to reschedule cannabis.
Out of all the quotes and statements flooding the cannabis media today, Rep. Earl Blumenauer (D-OR) best summarized the feelings shared by many folks in the industry: “This is a step in the right direction but it is not sufficient. I hope it is followed by more significant reforms. This is long overdue.”
The South African government has taken a leap into the future (ahead also of the expected World Health Organization (WHO) decision on cannabis this December). Namely, it has begun to regulate hemp (more in line with Europe intriguingly, than the U.S.) and attempted to remove the THC part of the equation from a domestic list of plants and drugs with no medical use.
The notice was signed by South African Minister of Health Zweli Mkhize and published a week after a domestic moratorium on CBD expired. The moratorium permitted the sale of some kinds of CBD products.
This is an intriguing new development, although it will also undoubtedly cause headaches for the burgeoning industry in the region.
On The CBD Front…
South Africa’s new hemp guidelines – namely for the amount of THC allowed in legit hemp crops that are also regulated – are that plants contain no more than 0.2% THC. This makes the guidelines absolutely in line with what is generally developing across the EU. And even more intriguingly, below federal guidelines for most U.S. domestic hemp crops (which are 0.3% at a federal level and only differ in a few state cases where the amount is lower by state law).
However, there is also a unique twist to all of this: The South African government has now created a two-pronged regulatory schemata just for CBD. The default approach to the cannabinoid is that it is in fact medication, scheduled under South African internal and global drug guidelines as a “Schedule 4” drug.
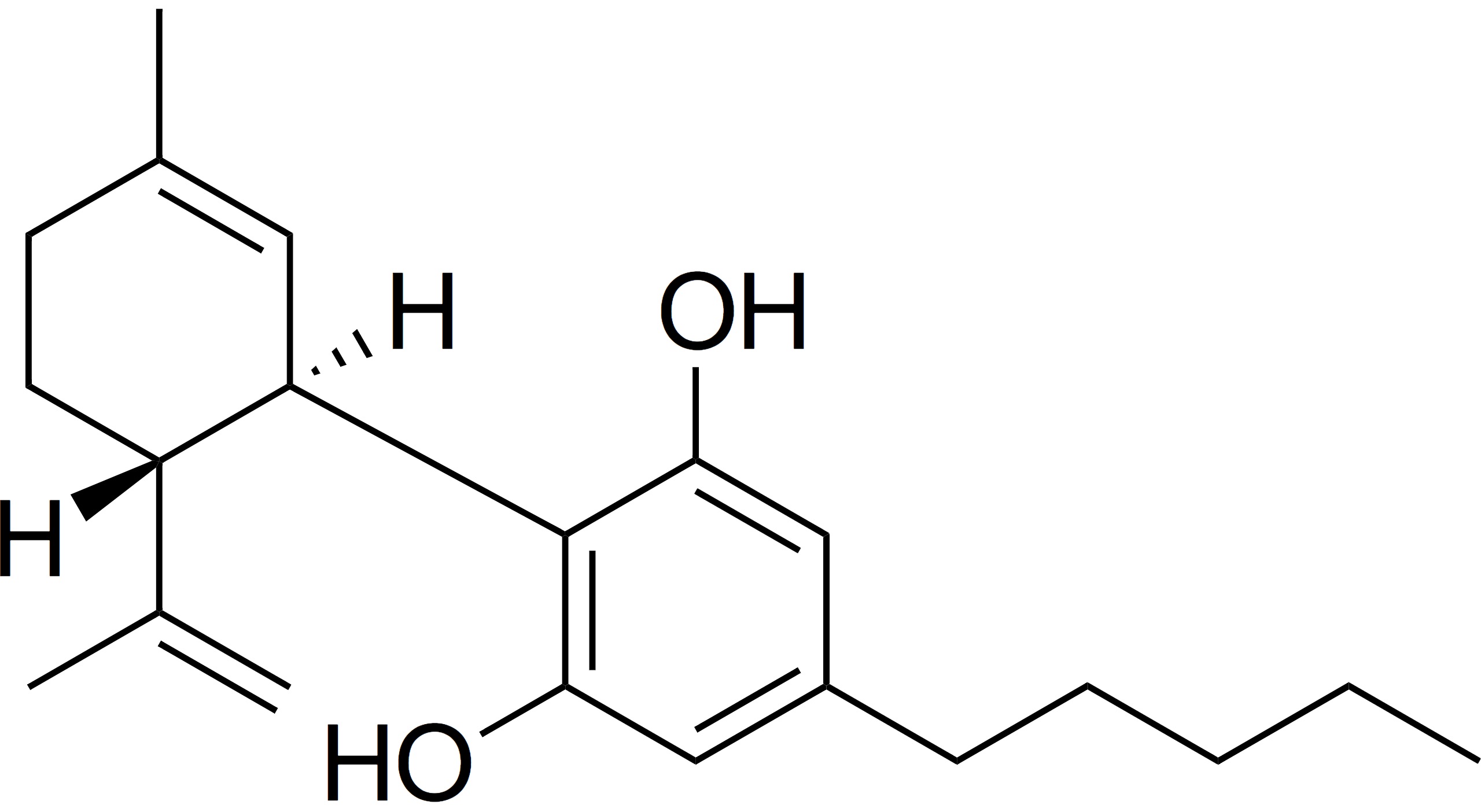
The structure of cannabidiol (CBD), one of 400 active compounds found in cannabis.
The other designation is reserved for CBD packaged in sizes of 600mg or less (and limited by instructions to no more than 20mg a day). This kind of CBD (despite the dubious understanding of cannabinoid science) will henceforth be labelled a “supplement” and on “Schedule 0”.
However, do not be fooled: This is not “descheduling.” This actually means that all CBD has been classified as a medical substance except in packets that are under a certain size, with portion suggestions on the outside of the wrapper or package.
That is hardly scientific. However, what is more burdensome is that any CBD cultivator in South Africa must also be GMP- (or internationally medically) certified (even if bound for the supplement market). By definition, in other words, it will make the cost of production for the supplement (commercial, food and cosmetic) part of the equation as expensive as pharmaceutical production. While from a purist’s point of view, having ultra clean cannabis in any product (at the level of pharmaceutical standards) is a wonderful idea, but this gets ridiculous when it comes to reality, and will ultimately never stand.
This development is also undeniably inconvenient (at minimum) for any who had envisioned outdoor hempires, which most of the cannabis grown in South Africa is. The only people who have the money to build indoor grows, starting with GMP certified greenhouses, are, for the most part, white people, foreigners or those who own property and have access to external, international equity.
The sins of Apartheid, in other words, are being writ large on the entire cannabis industry at present in South Africa. And CBD is contained right in the middle of the mix.
On The THC Front…
There are several interesting aspects to this.
The first is that THC has been removed from the South African “Schedule 7” which is roughly equivalent to the international “Schedule I” that cannabis also resides in until the WHO re- or deschedules the same.
However, this also means that all CBD as well as THC must be produced by those with pharmaceutical-grade facilities – and this of course includes more than just indoor, temperature-controlled greenhouses. It also includes a complex supply chain that is European and Western centric, starting with the requirement to access a rather large amount of capital to construct the same.
Global Re-Alignment Or Stopgap Measure?
This new regulation, in other words, specifically leaves the vast majority of what has already been seeded, or what is most likely to be, in the hands of a few Canadian and other companies who have been moving in this direction for the last several years.
It also implies, intriguingly, that the intra-African cannabis market is low priority at present for those writing the (health) rules. And that also means that eyes are being set more on creating an export market than for treating South African citizens.
It is not an unusual move, rather tragically so far. And almost certainly one that will be challenged, and in several directions, both by events, but also by firms caught up in the mix.
Why? For starters, the South African cannabis market also effectively controls the Lesotho cannabis regulatory scheme (namely all exports from Lesotho, which has seen quite a lot of cannabis investment over the last several years). All such crops must be labelled per South African guidelines if they, literally, can hit a port to be exported.
The vast majority of those grows, even with relatively decent foreign backing, are also outside – and of course as a result ineligible for GMP certification.
Of course given the fact that the UN is likely to clarify both the status of THC and CBD by the end of the year, this current situation in South Africa is also fairly clearly intended to be a stop-gap regulatory measure to last up until at least this time.
Where it may go after that is anyone’s guess. This measure, however, is also clearly being made to protect those who have invested in GMP-grade facilities as opposed to those who have been clearly angling for reform on the CBD front, starting with the beer market. Stay tuned. Interesting developments clearly ahead.
Under the U.S. Drug Enforcement Administration’s (DEA) Controlled Substance Act (CSA), drugs are classified into five distinct schedules depending upon their acceptable medical use and their overall potential for abuse or dependency. The DEA currently lists cannabis as a Schedule I drug, which the CSA defines as drugs having no currently accepted medical use and a high potential for abuse. It appears, however, that the DEA may soon reconsider its current Schedule I classification of cannabis.
This article considers how the DEA’s potential reclassification of cannabis potentially could affect Georgia’s medical cannabis industry. Specifically, the article discusses: (1) how Georgia medical cannabis distributors would operate within this new regulatory framework; (2) how this change would affect registered Georgia patients who are either currently purchasing medical cannabis or are planning to do so; and (3) whether this reclassification would cause big pharmaceutical companies to enter Georgia’s medical cannabis market, and if so, how.
The DEA’s Reclassification of Cannabis Would Likely Affect the Regulatory Framework of Georgia’s Medical Cannabis Industry
On April 2, 2019, Georgia became the 34th U.S. state to legalize cannabis for medicinal use when the Georgia Legislature passed House Bill 324 (“HB 324”), which recently took effect on Monday, July 1, 2019. In Georgia, medical cannabis is defined as a “low-THC oil” that contains 5% or less of tetrahydrocannabinol (THC)—the psychoactive chemical in cannabis that causes a “high.”
Georgia State Flag
If the DEA reclassifies cannabis, the regulatory framework of Georgia’s medical cannabis industry under HB 324 would likely be affected. For instance, depending on how the DEA elects to reclassify cannabis, low-THC oil products manufactured and sold in Georgia could become subject to the U.S. Food and Drug Administration’s (FDA) costly, complicated and time-consuming drug approval process. Then, any low THC oil products that the FDA approves will be subject to federally mandated quality, efficacy and potency standards for FDA-approved drugs. Also, any federal standards that stem from the DEA’s reclassification of cannabis will trump any conflicting provisions in HB 324 or any other conflicting rules, regulations or procedures established by the Georgia Access to Medical Cannabis Commission (GAMCC), the seven member state agency responsible for promulgating and implementing the state-based rules, regulations and procedures necessary to produce and distribute low-THC oil in Georgia, and the Georgia State Board of Pharmacy (Pharmacy Board). However, even if the DEA reclassifies cannabis, the following state regulatory framework established by HB 324 will remain unaffected:
The GAMCC will likely continue to oversee the state’s medical cannabis industry.
The following two different types of dispensary licenses issued under the legislation will still likely remain: retail outlets (issued by the GAMCC) and pharmacies (issued by the Pharmacy Board).
Licensed dispensaries will still likely not be located within a 1,000-foot radius of a school or church, and licensed production facilities will still not be located within a 3,000-foot radius of a school or church.
Pharmacists who dispense low-THC oil will still likely have to review each registered patient’s information on the state’s Prescription Drug Monitoring Program (PDMP) database to confirm that they have been diagnosed with one or more of the 17 approved conditions and diseases. The legislation does not require retail outlet dispensaries to review patient information on the PDMP database or employ a pharmacist to dispense the drug.
Registered patients will still likely be prohibited from vaping low-THC oil or inhaling it by any other electronic means. The legislation does not expressly prohibit the use of other, non-electronic delivery methods of low THC oil such as pills or nasal spray.
All licensed dispensaries (and all licensed production companies) will still likely be subject to an “on-demand” inspection when requested by the Georgia Bureau of Investigation (GBI), the GAMCC, the four-member Medical Cannabis Commission Oversight Committee (MCCOC), or local law enforcement. The GAMCC and the Georgia Drugs and Narcotics Agency (GDNA) will also still likely be able to conduct one, annual inspection of dispensary locations. And, upon request, licensed dispensaries will still likely be required to immediately provide a sample of their low-THC oil for laboratory testing to the GBI, GAMCC, MCCOC, GDNA or local law enforcement.
All licensed dispensaries (and all licensed production facilities) will still likely be required to utilize a GAMCC-approved seed-to-sale tracking software.
All licensed dispensaries (and all licensed production companies) will still likely be prohibited from advertising or marketing their low-THC oil products to registered patients or the public. However, they will still likely be allowed to provide information about their products directly to physicians, and upon request, physicians will still likely be allowed to furnish the names of licensed dispensaries (and licensed production companies) to registered patients or their caregivers.
The DEA’s Reclassification of Cannabis Would Likely Affect the Availability of Low THC Oil
To date, approximately 9,500 Georgians are registered with the state’s Low-THC Registry, which allows them to purchase low-THC oil from licensed dispensaries. Since the legislation’s passage, the number of registered patients has increased significantly and continues to steadily rise. If the DEA reclassifies marijuana, this patient number will likely increase at an even faster rate because the public will likely perceive reclassification as an acknowledgement by the federal government that marijuana possesses health and medicinal benefits. If that occurs, statewide demand for low THC oil could quickly outstrip the supply.
Georgia Gov. Brian Kemp Image: Georgia National Guard, Flickr
Under HB 324, the GAMCC is tasked with ensuring that the state has a sufficient number of retail outlet dispensaries across the state to meet patient demand but is limited to issuing only six production licenses. As the number of registered patients continues to grow, the GAMCC may be forced to recommend amendments to the statute allowing it to issue additional production licenses to increase the state’s supply of low THC oil, and depending on how many additional patients are added to the state’s Low-THC Registry, the GAMCC may also have to issue additional dispensary licenses to keep up with patient demand by relaxing the geographic limitations on locating dispensaries.
Thus, the DEA’s reclassification of cannabis likely would affect the amount of low THC oil available to registered patients in Georgia.
The DEA’s Reclassification of Cannabis Would Likely Cause Large Pharmaceutical Companies to Enter Georgia’s Medical Cannabis Market
Large pharmaceutical companies typically manufacture, market, sell and ship their products on a national and international scale. Given cannabis’ current status as a Schedule I drug under the CSA, these companies have largely steered clear of the burgeoning medical marijuana industry because of the inherent risk of violating federal law. If the DEA reclassifies cannabis, that risk will be diminished greatly, and the companies therefore will likely decide to enter the market by acquiring existing medical marijuana companies with established national or state-level medical cannabis brands.
If the DEA reclassifies cannabis, Georgia’s medical cannabis market will likely be affected in multiple ways.Depending on how the DEA reclassifies cannabis, low-THC oil in Georgia could be subject to stringent federal standards, including the FDA’s complex and expensive drug approval process. Georgia medical cannabis companies will likely not be accustomed to complying with such federal regulations. Large pharmaceutical companies, on the other hand, are very accustomed to dealing with the federal government, including FDA drug approval. So, if the DEA reclassifies marijuana, pharmaceutical companies will likely view reclassification as a tremendous opportunity to enter the Georgia market by leveraging their experience and institutional knowledge dealing with federal law to acquire or partner with a licensed Georgia cannabis company that has an established brand of low -HC oil.
Entering Georgia’s medical cannabis market won’t be easy, however, because HB 324 prohibits licensees from transferring their licenses for five years and requires that the original licensee be a Georgia business. But, HB 324 does not prohibit them from selling their businesses, which necessarily includes any licenses the business owns. Purchasing a licensed Georgia medical cannabis company requires payment of a production license business transfer fee. The fee for the first sale of a business with a Class 1 production license is $100,000 and the fee for a Class 2 license is $12,500. The fee for the second sale is $150,000 for a Class 1 production license, and $62,500 for a Class 2 license. The fee for the third and fourth sales is $200,000 for a Class 1 production license, and $112,500 for a Class 2 license.
Conclusion
If the DEA reclassifies cannabis, Georgia’s medical cannabis market will likely be affected in multiple ways. Specifically, depending on how the drug is reclassified, the regulatory framework for medical cannabis companies likely will change to include both state and federal requirements, potentially including the FDA’s complex drug approval process. Also, the amount of low-THC oil available for registered patients to purchase likely will be diminished precipitating the need for the GAMCC to modify the statute to allow for issuing additional production licenses and relaxing the geographic limitations on locating dispensaries. Finally, large pharmaceutical companies likely will attempt to enter Georgia’s medical cannabis market by purchasing existing, licensed Georgia companies that have established low-THC oil brands.
At this point in the end of prohibition, not even the United Nations (UN) or the World Health Organization (WHO) are immune to the great green wave sweeping the planet. Yet, lest anyone get too optimistic about developments at the nose bleed level of international drug reform, the newest round of headlines regarding “WHO cannabis reform” is hardly cause for celebration.
The Story At The International Level So Far
In documents obtained by Cannabis Industry Journal last fall, it appeared that cannabis reform of the serious kind had caught the eye of senior leaders at the WHO. Further, it also appeared that some kind of decisive action or declaration would be forthcoming by the end of the year.
Yet as reported at the end of January, such decisions appear to be headed for a tortoise speed approvals track. Yes, it appears that CBD will probably be descheduled, and from both the hemp and cannabis perspective. That should be good news to many who are caught in a raft of international standards that are confusing and all over the place on a country-by-country level. However, this will not be much of a boon to the industry in Europe, in particular, where the discussion is less over CBD but the source of it, and how distillates are used. From this perspective, the draft WHO documents will make no difference, except perhaps to speed the acceptance of CBD, and create clearer regulations around it.
On the THC front, the WHO appears to do nothing more than move cannabis squarely into international Schedule I territory. More interesting of course, is the intent of international regulators to keep cannabis very much in uncertain status while moving “pharmacized” versions of the same into Schedule III designation.
What Does The Opinion of The WHO Really Mean?
What this means is also still unclear except that those who want to sell to regulated medical and nonmedical markets have to get their products (whatever those are) registered as medicine or a legitimate consumer product in every jurisdiction and eventually at a regional level (see Europe). That is clearly underway right now by both the big Canadian and emerging Israeli entities in the market as well as savvy European players in both verticals. That said, it is also a game that is about to create a very interesting market for those who are able to produce cheap, but high-grade oils in particular.
What Does This Mean For The Future Of Flower?
On the medical front, Germany became the third country in the world to consider reimbursing flower via national healthcare. Of the three who have tried it to date so far (and it is unclear what Poland will do at this point longer term), Israel is inching away and Holland nixed the entire cannabis covered by insurance conversation at the same time Germany took it on. Where that plays out across Europe will be interesting, especially as the cost of production and end retail cost continues to drop. And doctor education includes information about “whole plant” vs. pre-prescribed “dosing” where the patient has no control. The reality in the room in Europe right now is that this drug is being used to treat people with drug resistant conditions. Dosing dramas in other words, will be in the room here for some time to come as they have in no other jurisdiction.
Beyond dosing and control issues that have as much to do with doctors as overall reform, flower is still controversial for other reasons. One, it is currently still being imported into Europe from highly remote and expensive import destinations. That will probably change this year because of both the cultivation bid and Israel’s aggressive move into the middle of the fray as well as widely expected ex-im changes that will allow imports from countries throughout Europe. However, in the meantime, this is one of the reasons that flower is so unpopular right now at the policy and insurance level. The other is that pharmacists in Germany are allowed to treat the flower as a drug that must be processed. In this case, that means that they are adding a significant surcharge, per gram, to flower because they grind it before they give it to patients.
How long this loophole will exist is unclear. However, what is also very clear is that oils in particular, will play a larger and larger role in most medical markets. Read, in other words, “pharmaceutical products.”
For this reason, the WHO recommendations, for one, are actually responding to unfolding realities on the ground, not leading or setting them.
Setting A Longer-Term Date For Widespread Recreational Reform
This conservative stance from the WHO also means, however, that in the longer run, individual country “recreational reform” particularly in places like Europe, will be on a slower than so far expected track. There are no countries in the EU who are willing to step too far ahead of the UN in general. That includes Luxembourg, which so far has made the boldest predictions about its intentions on the recreational front of any EU member. However, what this also may signal is that the UN will follow the lead set by Luxembourg. Even so, this legitimately puts a marker in the ground that at least Europe’s recreational picture is at least five years off.
In the meantime, the WHO recommendations begin to set international precedent and potentially the beginnings of guidelines around a global trade that has already challenged the UN to change its own regulations. In turn, expect these regulations to guide and help set national policy outside a few outliers (see Canada, Uruguay and potentially New Zealand) globally.
Bottom line, in other words? The latest news from the UN is not “bad” but clearly seems to say that cannabis reform is a battle that is still years in the making. That said, from the glass is half full perspective, it appears, finally, there might be the beginning of a light at the end of the international tunnel of prohibition.
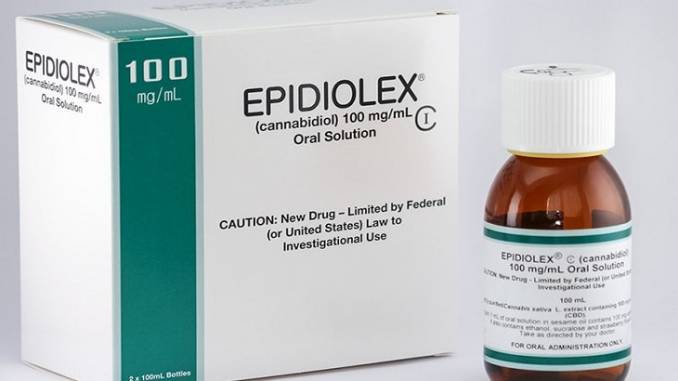
In a fascinating early August conference call with Seeking Alpha, British-based GW Pharmaceuticals finally revealed their retail price point for CBD-based drug, Epidiolex, as it goes into distribution in the U.S.
The ineffectiveness of GW Pharma’s drugs for many patients (along with the cost charged for them) was responsible for pre-empting the entire access discussion in the UK this year. The mother of an epileptic British child tried to import a personal store of cannabis oil (produced by Canadian LP Tilray) only to have it confiscated at the airport this summer. Her son ended up in the hospital shortly thereafter.
The majority of this cost will not be picked up by private health insurers but rather the federal governmentActually, according to industry analysis, this is about 70% more than the price of one comparable drug (Onfi), and slightly more expensive than Banzel, the two competing (non-cannabinoid based) medications now available in the U.S. for this market.
Here is the other (widely unreported) kicker. The majority of this cost will not be picked up by private health insurers but rather the federal government, which is also not negotiating with GW Pharma about that high price (unlike for example what is going on in Europe and the German bid).
Why the difference?
Two reasons. The first is that Epidiolex has obtained “orphan drug” status (a medication for a disease that affects fewer than 200,000 patients in the U.S.) The second is that the majority of the insurance that will be picking up this tab is Medicaid. The patient pool will be unable to afford this. As a result, the bulk of the money will remit not from private insurance companies but rather federal taxpayers. And, unlike in say, Germany, none of this is pre-negotiated in bulk.
What is the price of Epidiolex? $32,500 per patient, per year.
Co-payments are expected to range from $5 to $200 per month per patient after insurance (read: the government) picks up the tab. This essentially means that the company plans to base participation at first at least on a sliding scale, highly subsidized by a government that has yet to reschedule cannabis from a Schedule I in the U.S.
Creating, in other words, a new monopoly position for GW Pharmaceuticals in North America.
A Hypocrisy Both Patients And The Industry Should Fight
The sordid, underhanded politicking that has created this canna monster is hardly surprising given the current political environment in both the U.S. and the U.K. right now. The people who benefit the most from this development are not patients, or even everyday shareholders, not to mention the burgeoning legitimate North American cannabis industry, but in fact highly placed politicians (like British Prime Minister Theresa May). Philip May, the PM’s husband’s firm is the majority shareholder in GW Pharma. Her former drugs minister (with a strong stand against medical cannabis) is married to the managing director of British Sugar, the company that grows GW Pharma’s cannabis stock domestically.
So far, despite a domestic outcry over this in the UK (including rescheduling), there has been no political backlash in the United States over this announcement. Why not?
Look To Europe For A More Competitive Medical Market
This kind of pricing strategy is also a complete no go in just about every other market – including medical-only markets where GW Pharma already has a footprint.
For example, German health insurers are already complaining about this kind of pricing strategy for cannabis (see the Cannabis Report from one of the country’s largest insurers TK – out earlier this year). And this in an environment where the government, in fact, does negotiate a bulk rate for most of the drugs in the market. Currently most German cannabis patients are being given dronabinol, a synthetic form of THC which costs far less.
On top of this, there are also moves afoot by the German government to begin to bring the costs of medical cannabis and medicines down, dramatically. And this too will impact the market – not only in Europe, but hopefully spark a debate in every country where prices are also too high.
The currently pending German cultivation bid for medical cannabis has already set an informal “reference” price of at most 7 euros a gram (and probably will see bid competitors come in at under half that). In other words, the government wholesale price of raw, unprocessed cannabis flower if not lightly processed cannabis oil is expected to be somewhere in the neighbourhood of 3-4 euros per gram come early next year. If not, as some expect, potentially even lower than that.
Processed Cannabis Medicine vs. Whole Plant Treatment
The debate that is really raging, beyond pricing, is whether unprocessed cannabis and cannabis oil is actually “medicine.” At the moment, the status quo in the U.S. is that it is not.
GW Pharmaceuticals, in other words, a British company importing a CBD-based derivative, is the only real “medical cannabis” company in the country, per the FDA. Everyone else, at least according to this logic, is placed in the “recreational camp.” And further, hampered still, with a lack of rescheduling, that affects everyone.
If that is not an organizing issue for the American cannabis industry, still struggling with the many issues inherent in the status quo (from insurance coverage and banking to national distribution across state lines) leading up to the midterms, nothing will be.
As many probably already know, last month the DEA announced that the organization was going to reconsider its position on cannabis and would come to a decision about whether or not to reschedule cannabis on The Controlled Substance Act (CSA) by June of this year. Many would say this is long overdue, considering the DEA has cannabis listed as a Schedule I drug, the same as heroin and LSD.
Rescheduling cannabis to Schedule II would place it in the same category as Vicodin, cocaine, methamphetamine, Adderall, oxycodone, and many more. These substances are defined as drugs with a high potential for abuse, with use potentially leading to severe psychological or physical dependence. However, they are recognized as having some potential medical benefits.
If cannabis were to become a Schedule II drug, it would allow further research on the plant. This could be beneficial to the industry because further medical research would finally provide the scientific validation that cannabis does have medical benefits and that it should be accepted as a form of medicine.
Those benefits come with a steep cost.
If cannabis becomes Schedule II it means the federal government finally sees cannabis as a plant (drug) that can provide some medical value. Which, at face value, is good because that is what many advocates have been fighting for. On the other hand, the only reason that larger pharmaceutical companies have largely kept out of the industry so far is because it is a Schedule I drug and the government did not officially recognize that it had any medical value. If this were to change, there is no reason for those pharmaceutical companies to continue watching from the sidelines. There is also no industry better fit than the pharmaceutical industry to run, manufacture, control, and profit from medical cannabis. The infrastructure is already in place.
There is also not another industry that has the money and the historical relationship with the FDA like the pharmaceutical industry. If the FDA were to regulate cannabis, it would have to regulate every single product on the shelf of every single dispensary, which would require more stringent lab testing guidelines. Just because one of your brownies made it through the FDA regulation process, does not mean the cookie next to it will. Entering into this process would take companies years to complete and cost more than $1 billion per product. Think about how many products some dispensaries have. Think about the number of different strains that dispensaries carry. That requires years of testing and multiple billions of dollars, just for the strains.
Big Pharma is positioned perfectly to come in and take control of the entire process if this happens. It will be a mad rush from all pharmaceutical companies to come in and quickly obtain market share. I know that as an industry we think we are seeing a lot of money in sales and profit, but compared to the pharmaceutical industry, it is merely a drop in the bucket. These companies will easily, and willingly, out-spend every company currently in the industry to the point where we can no longer compete. All the work that advocates and business professionals have put in to get the industry to where it is today could be lost.
Schedule II status would also turn the adult-use industry into utter chaos. The only reason we are able to have an adult-use market right now without the interference of the FDA is because cannabis is federally illegal. If cannabis is moved to Schedule II it will be recognized by the government, which means the FDA will have to come in and start the approval process for every product on the shelf. How smoothly do you think that will go for the adult-use retail centers in the industry? The cost alone will force shops to close. There is also not another substance that has a Schedule II classification that we have an adult-use industry for. Could cannabis be the first? I would not want to take that chance with the government or have to go through that process as an adult-use cannabis business owner.
When discussing this matter with several colleagues, some would ask “But what about now? We are in direct violation of the federal law right now, and they are leaving us be.”
Yes, that is for the most part true, but it is true because cannabis is now a Schedule I, federally illegal drug. Meaning the government does not even recognize it. The FDA will not regulate anything that is not recognized by the federal government because they are a federal agency. If the FDA were to implement regulations and an approval process, that would mean that a federal agency is recognizing cannabis as a consumer product. Right now that goes directly against the government’s public stance on the issue. And pharmaceutical companies cannot start selling a drug that is federally illegal and has been classified by the government as having no medical value. But as soon as the government recognizes cannabis as a form of medicine, it opens the doors for these organizations to get involved because it is justifiable now.
If that were to happen all the money that has been generated in this industry, and has made several people very wealthy and successful, will slowly, but surely get stuffed into the pockets of Big Pharma, the FDA and the government.
In my mind, rescheduling cannabis to a Schedule II substance will create more issues for the industry than it will benefits.
If the government were to take any stance on cannabis, it should completely declassify it. It should not be listed on any type of controlled substance list by the government. It is a natural plant, not a man-made substance. If the government will not declassify cannabis, I would rather them keep it as a Schedule I substance. At least this way it protects the industry and keeps it as is, belonging to the people.
Opportunities like the cannabis industry are once in a lifetime. It would be a shame to see it taken by Big Pharma, or controlled by the government.
For those that have made it this far down on this post, please understand that this is a worst-case scenario. A very drastic, but realistic outcome down one of the many paths the industry could go. But the motto in this industry since the beginning was, “prepare for the worst, and pray for the best.” I think we should follow those instructions now more than ever.
Editor’s Note: This article represents the opinion of the author, not necessarily that of Cannabis Industry Journal. We invite all readers who agree or disagree with the author’s opinion to join the conversation in the comments section below the article.
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
We use tracking pixels that set your arrival time at our website, this is used as part of our anti-spam and security measures. Disabling this tracking pixel would disable some of our security measures, and is therefore considered necessary for the safe operation of the website. This tracking pixel is cleared from your system when you delete files in your history.
We also use cookies to store your preferences regarding the setting of 3rd Party Cookies.
If you disable this cookie, we will not be able to save your preferences. This means that every time you visit this website you will need to enable or disable cookies again.

 Many cannabis stocks across the market saw significant spikes in trading prices following the news of the recommendation. Industry stakeholders and trade organizations seem to share a similar sentiment across the board: Not quite exuberance and celebration, but cautious optimism. The move doesn’t mean the federal government is legalizing cannabis, but they are showing their willingness to work with the industry.
Many cannabis stocks across the market saw significant spikes in trading prices following the news of the recommendation. Industry stakeholders and trade organizations seem to share a similar sentiment across the board: Not quite exuberance and celebration, but cautious optimism. The move doesn’t mean the federal government is legalizing cannabis, but they are showing their willingness to work with the industry. Importantly, the move would remove the dreaded 280E tax burden that has plagued the cannabis industry with huge tax penalties. It would also lift many barriers to study cannabis that have hindered research for decades.
Importantly, the move would remove the dreaded 280E tax burden that has plagued the cannabis industry with huge tax penalties. It would also lift many barriers to study cannabis that have hindered research for decades.